Direct and Indirect Associations of Sociodemographic Factors and Patient-Perceived Barriers With Delayed Breast Cancer Presentation: A Cross-Sectional Path Analysis
DOI:
https://doi.org/10.14740/wjon2754Keywords:
Breast cancer, Patient-perceived barriers, Delay presentation, Path analysisAbstract
Background: Delayed presentation remains a contributor to advanced-stage breast cancer (BC) diagnosis and poor outcomes. Although sociodemographic factors are known to influence presentation delay, patient-perceived barriers may play a role in help-seeking behavior. However, the association linking sociodemographic characteristics, patient-perceived barriers, and delayed presentation remains insufficiently understood. This study aimed to examine the direct and indirect associations between sociodemographic factors, patient-perceived barriers, and delayed BC presentation using a path analysis approach.
Methods: This cross-sectional study included 150 women with BC. Sociodemographic characteristics, presentation interval, and patient-perceived barriers were collected through medical records and semi-structured interviews. Patient-perceived barriers were identified through content analysis of open-ended responses. Path analysis was conducted to estimate direct, indirect, and total effects.
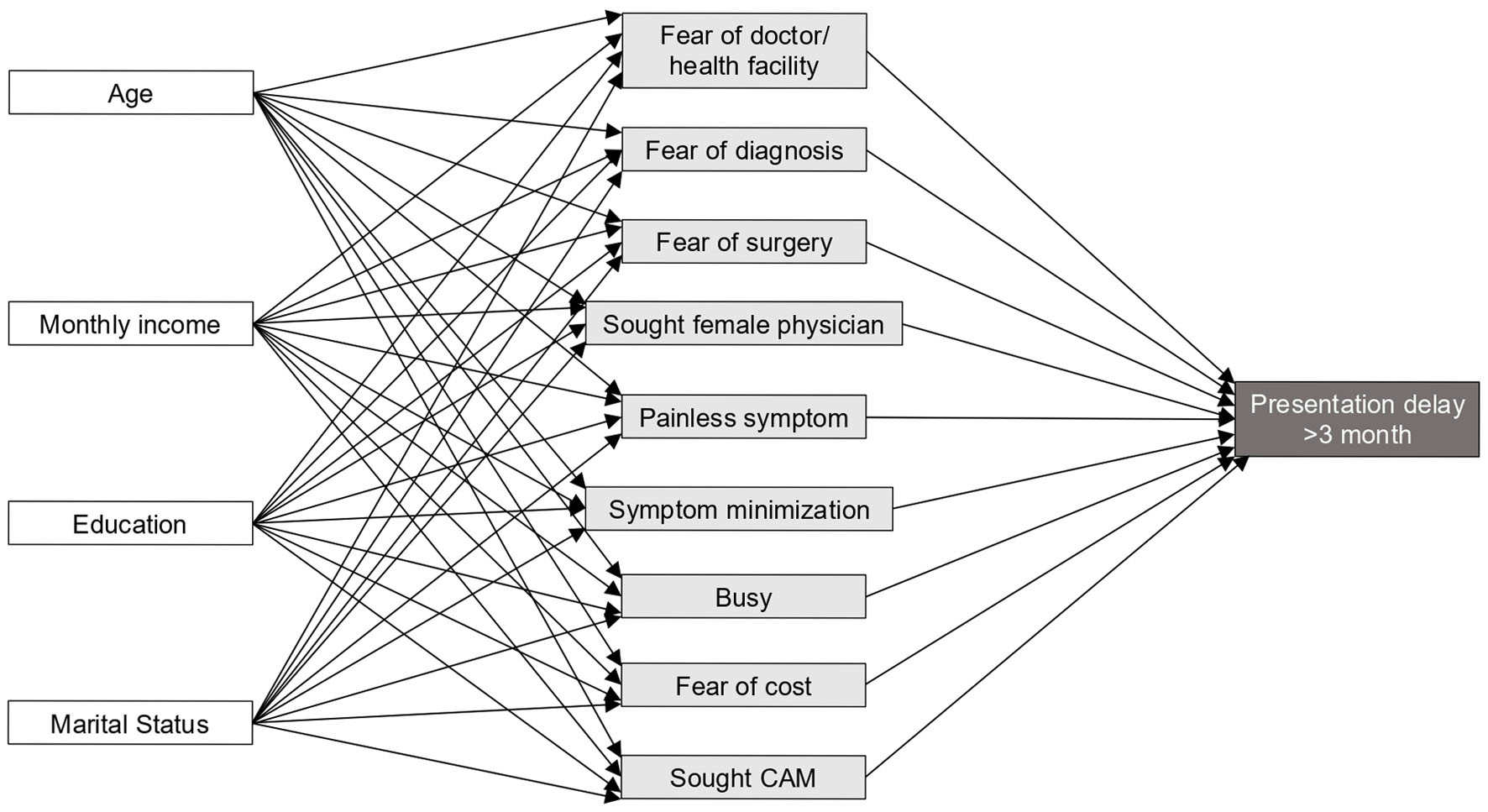
Results: None of the total indirect effects from sociodemographic variables to presentation delay through patient-perceived barriers were statistically significant. Five specific indirect pathways tested using the joint-significance approach were also non-statistically significant: age through fear of surgery (β = −0.002; P = 0.149), monthly income through fear of diagnosis (β = −0.029; P = 0.116), monthly income through fear of surgery (β = 0.047; P = 0.087), monthly income through preference for a female physician (β = 0.026; P = 0.135), and education through fear of surgery (β = 0.072; P = 0.051). Several sociodemographic factors showed significant direct associations with specific patient-perceived barriers. Increasing age was associated with lower fear of visiting health facilities (β = −0.245; P < 0.05) and lower fear of surgery (β = −0.149; P < 0.05). Higher income was associated with lower fear of diagnosis (β = −0.128; P < 0.05), higher fear of surgery (β = 0.170; P < 0.05), and greater preference for female physicians (β = 0.161; P < 0.05). Lower educational attainment was associated with higher fear of surgery (β = 0.283; P < 0.01), while unmarried status was associated with higher fear of healthcare costs (β = 0.383; P < 0.01) and lower likelihood of seeking complementary and alternative medicine (β = −0.130; P < 0.05). Several patient-perceived barriers were directly associated with delayed presentation, including fear of diagnosis (β = 0.165; P < 0.01), fear of surgery (β = 0.247; P < 0.01), painless symptoms (β = 0.367; P < 0.001), symptom minimization (β = 0.105; P < 0.05), perceived busyness (β = 0.244; P < 0.01), and preference for female physicians (β = 0.105; P < 0.05).
Conclusion: Although the hypothesized mediation of sociodemographic factors by patient-perceived barriers was not supported, several sociodemographic factors were associated with distinct barrier profiles, and several patient-perceived barriers were associated with delayed presentation. These findings highlight the importance of addressing modifiable barriers to promote earlier presentation and improve BC outcomes.
Published
Issue
Section
License
Copyright (c) 2026 The authors

This work is licensed under a Creative Commons Attribution 4.0 International License.