| World Journal of Oncology, ISSN 1920-4531 print, 1920-454X online, Open Access |
| Article copyright, the authors; Journal compilation copyright, World J Oncol and Elmer Press Inc |
| Journal website https://wjon.elmerpub.com |
Original Article
Volume 17, Number 4, August 2026, pages 454-462

Direct and Indirect Associations of Sociodemographic Factors and Patient-Perceived Barriers With Delayed Breast Cancer Presentation: A Cross-Sectional Path Analysis
Juan Adrian Wiranataa ![]() , Susanna Hilda Hutajulub, f
, Susanna Hilda Hutajulub, f ![]() , Yufi Kartika Astarib
, Yufi Kartika Astarib ![]() , Angelica Abigaelc
, Angelica Abigaelc ![]() , Mardiah Suci Hardiantib
, Mardiah Suci Hardiantib ![]() , Kartika Widayati Taroeno-Hariadib
, Kartika Widayati Taroeno-Hariadib ![]() , Johan Kurniandab
, Johan Kurniandab ![]() , Yayi Suryo Prabandarid, e
, Yayi Suryo Prabandarid, e ![]() , Ibnu Purwantob
, Ibnu Purwantob ![]()
aDepartment of Internal Medicine, Faculty of Medicine, Public Health and Nursing, Universitas Gadjah Mada, Yogyakarta, Indonesia
bDivision of Hematology and Medical Oncology, Department of Internal Medicine, Faculty of Medicine, Public Health and Nursing, Universitas Gadjah Mada/Dr. Sardjito General Hospital Yogyakarta, Indonesia
cSanta Maria Hospital, Cilacap, Indonesia
dDepartment of Health Behaviour, Environment, and Social Medicine, Faculty of Medicine, Public Health and Nursing, Universitas Gadjah Mada, Yogyakarta, Indonesia
eCenter of Health Behaviour and Promotion, Faculty of Medicine, Public Health and Nursing, Universitas Gadjah Mada, Yogyakarta, Indonesia
fCorresponding Author: Susanna Hilda Hutajulu, Division of Hematology and Medical Oncology, Department of Internal Medicine, Faculty of Medicine, Public Health and Nursing, Universitas Gadjah Mada/Dr. Sardjito General Hospital, Yogyakarta 55284, Indonesia
Manuscript submitted February 27, 2026, accepted May 25, 2026, published online June 25, 2026
Short title: Barriers to Breast Cancer Presentation
doi: https://doi.org/10.14740/wjon2754
| Abstract | ▴Top |
Background: Delayed presentation remains a contributor to advanced-stage breast cancer (BC) diagnosis and poor outcomes. Although sociodemographic factors are known to influence presentation delay, patient-perceived barriers may play a role in help-seeking behavior. However, the association linking sociodemographic characteristics, patient-perceived barriers, and delayed presentation remains insufficiently understood. This study aimed to examine the direct and indirect associations between sociodemographic factors, patient-perceived barriers, and delayed BC presentation using a path analysis approach.
Methods: This cross-sectional study included 150 women with BC. Sociodemographic characteristics, presentation interval, and patient-perceived barriers were collected through medical records and semi-structured interviews. Patient-perceived barriers were identified through content analysis of open-ended responses. Path analysis was conducted to estimate direct, indirect, and total effects.
Results: None of the total indirect effects from sociodemographic variables to presentation delay through patient-perceived barriers were statistically significant. Five specific indirect pathways tested using the joint-significance approach were also non-statistically significant: age through fear of surgery (β = −0.002; P = 0.149), monthly income through fear of diagnosis (β = −0.029; P = 0.116), monthly income through fear of surgery (β = 0.047; P = 0.087), monthly income through preference for a female physician (β = 0.026; P = 0.135), and education through fear of surgery (β = 0.072; P = 0.051). Several sociodemographic factors showed significant direct associations with specific patient-perceived barriers. Increasing age was associated with lower fear of visiting health facilities (β = −0.245; P < 0.05) and lower fear of surgery (β = −0.149; P < 0.05). Higher income was associated with lower fear of diagnosis (β = −0.128; P < 0.05), higher fear of surgery (β = 0.170; P < 0.05), and greater preference for female physicians (β = 0.161; P < 0.05). Lower educational attainment was associated with higher fear of surgery (β = 0.283; P < 0.01), while unmarried status was associated with higher fear of healthcare costs (β = 0.383; P < 0.01) and lower likelihood of seeking complementary and alternative medicine (β = −0.130; P < 0.05). Several patient-perceived barriers were directly associated with delayed presentation, including fear of diagnosis (β = 0.165; P < 0.01), fear of surgery (β = 0.247; P < 0.01), painless symptoms (β = 0.367; P < 0.001), symptom minimization (β = 0.105; P < 0.05), perceived busyness (β = 0.244; P < 0.01), and preference for female physicians (β = 0.105; P < 0.05).
Conclusion: Although the hypothesized mediation of sociodemographic factors by patient-perceived barriers was not supported, several sociodemographic factors were associated with distinct barrier profiles, and several patient-perceived barriers were associated with delayed presentation. These findings highlight the importance of addressing modifiable barriers to promote earlier presentation and improve BC outcomes.
Keywords: Breast cancer; Patient-perceived barriers; Delay presentation; Path analysis
| Introduction | ▴Top |
Breast cancer (BC) is one of the most common malignancies in women worldwide. In Indonesia, BC accounts for 30.9% of women’s cancer cases and 11% of cancer deaths in 2020 [1]. In Yogyakarta Province, BC affects mostly younger women and often presents at advanced stages [2]. A local study reported a 5-year overall survival rate of 51% [3], lower than in nearby Asian countries.
Delays in presentation can impede early identification and diagnosis of BC, which in turn increases the burden of advanced-stage disease at initial presentation and ultimately results in poorer prognosis and reduced survival. Numerous studies found that factors such as lower education, older age, lower socioeconomic status, rural residence, and limited healthcare access are associated with delay in presentation [2, 4, 5]. Consequently, these delays lead to worse outcomes and add considerable constraints to the healthcare system, which must then provide more complex, intensive treatment.
Presentation delay might also be caused by factors beyond sociodemographic and clinical determinants, as evidence suggests that patient-perceived barriers play a pivotal mediating role in shaping help-seeking behavior. Barriers include the perception of a painless symptom, the attribution of symptoms to a non-serious condition (symptom minimization), fear of cancer diagnosis, and fear of surgical procedures [2, 4]. All are observed to significantly affect cognitive appraisal and emotional processing, potentially leading to delayed recognition of symptom seriousness and delayed medical consultation. Understanding these internal psychological and cognitive barriers is essential for developing targeted interventions that encourage timely presentation and improve BC outcomes.
One method that might offer a valuable methodological approach for examining the role of patient-perceived barriers as mediators between sociodemographic factors and presentation delay is path analysis. Path analysis allows for the simultaneous estimation of direct, indirect, and total effects among multiple variables within a hypothesized causal framework. Path analysis might help assess whether sociodemographic characteristics indirectly influence delays through their association with patient-perceived barriers, providing insight into complex relationships among determinants and enabling distinction of the contributions of mediating variables. Moreover, this analysis is well-suited for testing theoretical models of health behavior, thereby helping clarify the associations underlying delays in presentation [6].
This study aimed to examine the direct and indirect associations between sociodemographic factors, patient-perceived barriers as reasons for delay, and delayed BC presentation through path analysis, which may provide an understanding of how these factors interact among BC patients and identify possible actionable targets for intervention that could promote earlier presentation and improve outcomes.
| Materials and Methods | ▴Top |
Study participants and data collection
Subjects were retrospectively recruited from a primary study that aimed to analyze chemotherapy-related toxicity and its impact on survival in 250 patients with BC. The study was conducted at the Hematology and Medical Oncology Division, “Tulip”/Integrated Cancer Clinic, Dr. Sardjito General Hospital, Yogyakarta, Indonesia, between July 2018 and March 2022. Eligible subjects were women aged 18 or older with histopathologically confirmed BC and an Eastern Cooperative Oncology Group (ECOG) performance status of 0 or 1. Subjects with terminal illness, severe comorbidities, or those unable to provide accurate information due to psychotic disorders or any other causes were excluded to mitigate potential limitations in recall and interview coherence, as well as to avoid causing undue distress to these vulnerable groups.
A semi-structured questionnaire was developed to collect sociodemographic data, presentation delay, and reasons for delay, as described in detail in the previous study [2]. During development, three independent general practitioners performed forward and backward translations into Bahasa Indonesia. The questionnaire was then assessed for face validity through a pilot test with six individuals without a medical background. These participants were convenience sampled via contacts known to the research team. Trained research team members conducted face-to-face interviews from September 2020 to February 2021. Seventy-seven interviews occurred at the clinic. Due to the COVID-19 pandemic and travel restrictions, 74 interviews took place by phone. The study received ethical approval from the Faculty of Medicine, Public Health, and Nursing of Universitas Gadjah Mada/Dr. Sardjito General Hospital Joint Ethics Committee (Reference Number: KE/FK/0444/EC/2020). The study was conducted in compliance with the ethical standards of the responsible institution on human subjects as well as with the Helsinki Declaration.
Study variables
Participant age was defined at BC diagnosis. Monthly income included individual or household earnings and was classified as ≤ 3 million Rupiah or > 3 million Rupiah (referred to as an income cut-off for happiness index > 70 by the Indonesian Ministry of National Development Planning in 2021 [7]). Educational attainment was measured as the highest level of formal education completed, categorized as senior high school or higher (including a bachelor’s degree or higher), and no formal education or only primary or junior high school. Marital status was dichotomized as married or single, widowed, and divorced.
The presentation duration interval was defined as the time from initial BC symptom onset to the patient’s first visit to a health facility or medical professional (doctor, nurse, or midwife). During the interview, subjects were asked about the date of symptom onset and the date of their first consultation. If participants could not recall exact dates, uncertain dates were handled using a procedure adapted from the Cancer Symptom Interval Measure (C-SIM) protocol for calculating “pseudo-exact” dates from estimated dates. First, participants were encouraged to estimate the period in months. Interviewers then helped refine these estimates by linking them to notable occasions or holidays to narrow the date range. If only a month was given, follow-up questions aimed to find the exact day or relate it to events within that month. Documented surgery dates in clinical records were used as benchmarks, as these were often key milestones for patients. When exact dates were unknown, participants were asked to provide a month or a month range, along with the year. If only a month was provided, the 15th was used as the estimated date; for a range of months, the midpoint between the 15th of those months was used. If only the year were available, June 30 was used as the estimated date [3, 4, 8].
Presentation delay was then determined based on the presentation duration interval, with intervals of more than 3 months considered delayed presentations, in accordance with previous literature [3, 4]. To address patient-perceived barriers, open-ended questions were included to elicit subjects’ reasons for delaying presentation.
Statistical analysis
A content analysis of the interview transcripts was conducted to assess patient-perceived barriers, based on participants’ open-ended responses to the question of delayed presentation [9]. Two research team members independently generated inductive codes without a predetermined framework. Codes were compared, collated, and refined into candidate themes representing patient-perceived barriers. Discrepancies were resolved by consensus with consultation with a third research team member. Themes were then defined and named accordingly. The theme with only one response was excluded because it captured only prominent and recurring patterns of patient-perceived barriers [9, 10]. Descriptive analysis was performed to observe the distribution of subjects’ characteristics. Subject characteristics were summarized using mean and standard deviation (SD), median, or frequencies as appropriate.
Path analysis was conducted using structural equation modeling with maximum likelihood estimation to examine the hypothesized causal pathway linking sociodemographic variables to presentation delay, mediated by patient-perceived barriers (Fig. 1). Path analysis is a subset of structural equation modeling that enables the estimation of regression coefficients corresponding to the direct, indirect, and total effects among variables. It is beneficial for testing theoretical models that propose causal relationships between a set of observed variables. The beta estimates in our path analysis represent standardized regression coefficients and are interpreted similarly to beta estimates obtained from generalized linear models, indicating the expected change in a dependent variable for a one-unit change in the independent variable [6]. To explore the possibility of pathway-specific mediation, following the joint-significance approach to mediation testing [11], specific indirect effects were estimated for the subset of candidate pathways in which both constituent direct paths were statistically significant.
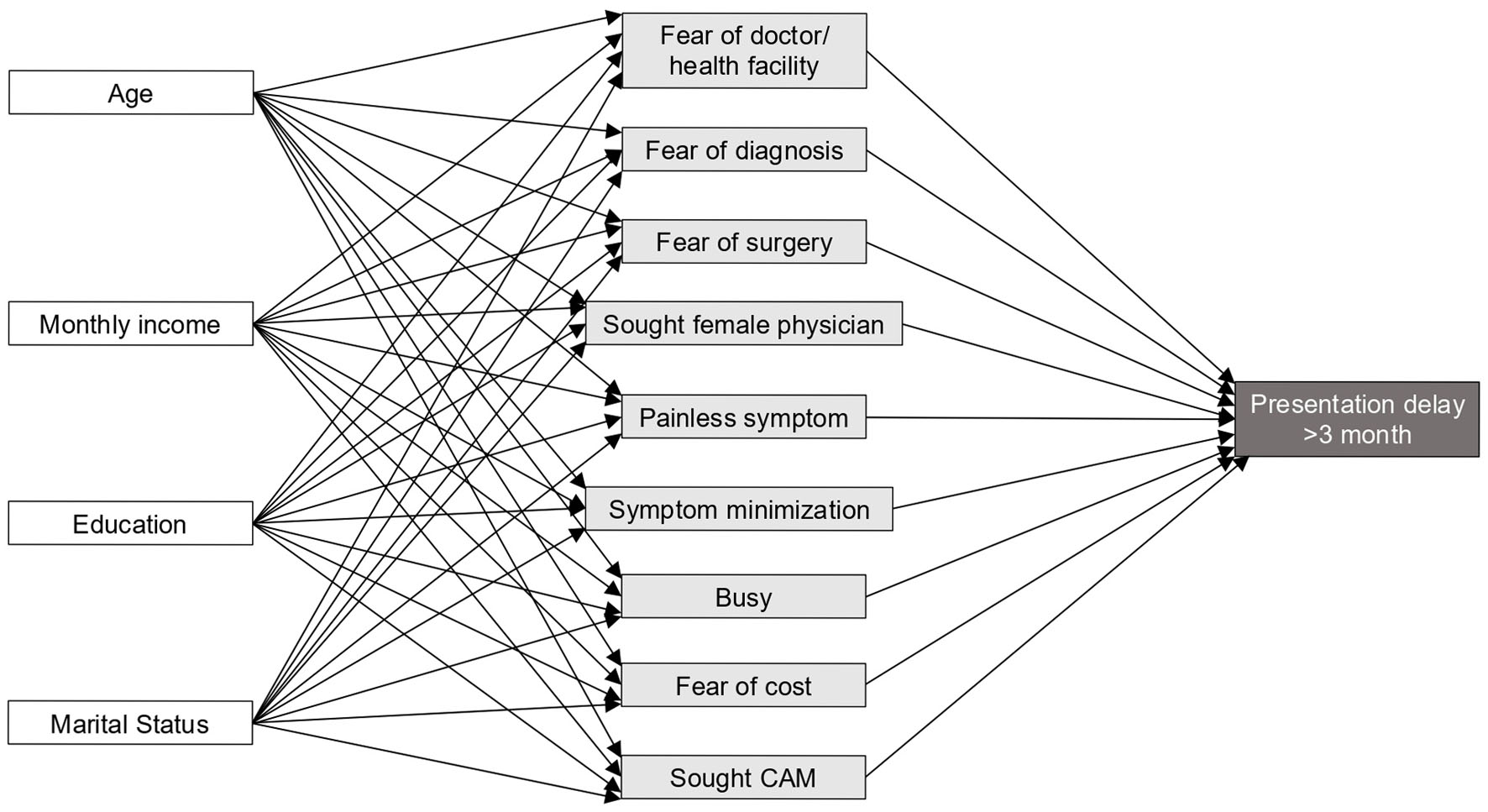 Click for large image | Figure 1. Hypothesized pathways between sociodemographic variables and presentation delay. White boxes represent sociodemographic variables, light gray boxes represent patient-perceived barrier mediators, and the dark gray box represents presentation delay of more than 3 months. |
A P-value of < 0.05 was considered statistically significant. Model fit was evaluated using the root mean square error of approximation (RMSEA), standardized root mean square residual (SRMR), Comparative Fit Index (CFI), and Tucker–Lewis Index (TLI) [6]. Bootstrapped standard errors and corresponding 95% confidence intervals (CIs) were computed using 1,000 replicates. All statistical analyses were carried out using STATA software version 17 (StataCorp, College Station, TX).
| Results | ▴Top |
Study participants
A total of 214 patients had been registered in the main study. Of these, three dropped out, and 38 had died. Among the 173 eligible patients, 16 did not respond to the invitation, and six declined to participate. One patient was excluded due to an inability to recall information or communicate effectively during the interview. In total, 150 patients were included in the final analysis.
The mean age of the participants was 53.2 years. The majority of participants were aged ≤ 60 years (80.7%), reported a monthly income of less than 3 million IDR (70.0%), attained formal education from senior high school to higher degree (57.3%), were married (83.3%), and experienced a presentation delay of ≤ 3 months (55.3%). Reasons for delay as patient-perceived barriers identified in the analysis were painless symptom (28.7%; attributed their delay in seeking care to symptoms experienced not associated with any pain or physical discomfort) and symptom minimization (22.7%; the attribution of symptoms to a non-serious condition), followed by fear of surgery (15.3%), perceived busyness (11.3%), fear of doctor or health facility visit (4.7%), sought complementary and alternative medicines (CAM) (4.0%), fear of diagnosis (4.0%), fear of cost (2.7%), and sought female physician (Table 1).
 Click to view | Table 1. Study Characteristics (N = 150) |
Path estimates and mediation
Our model depicting the relationships among sociodemographic variables, patient-perceived barriers, and presentation delay is shown in Figure 2. The model fit indices of RMSEA of 0.064 and SRMR of 0.063 suggest an acceptable fit. However, the indices of CFI of 0.732 and TLI of 0.430 were under the threshold for adequate fit. The direct, total indirect, and specific indirect effects of sociodemographic variables on presentation delay of more than 3 months, mediated by patient-perceived barriers, are presented in Supplementary Material 1 (wjon.elmerpub.com).
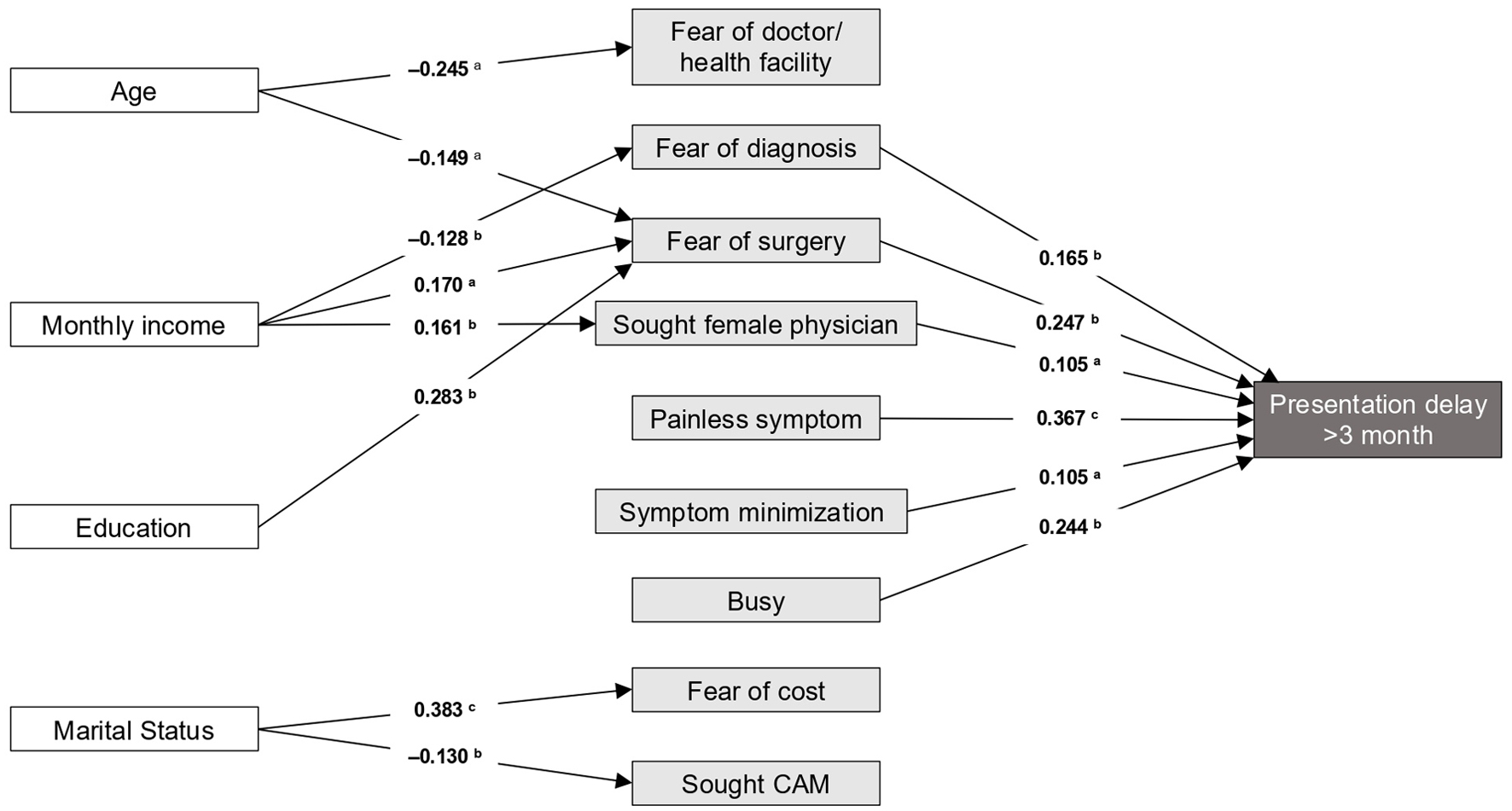 Click for large image | Figure 2. Path analysis for the relationship sociodemographic variables and presentation delay. aP < 0.05; bP < 0.01; cP < 0.001. |
None of the total indirect effects from the four sociodemographic variables to presentation delay reached statistical significance: age (β = −0.003, 95% CI −0.008, 0.003), monthly income (β = 0.145, 95% CI −0.087, 0.116), educational attainment (β = 0.066, 95% CI −0.041, 0.173), and marital status (β = 0.083, 95% CI −0.055, 0.221). The estimation of specific indirect effects using the joint-significance approach revealed that none of the five specific indirect pathways reached statistical significance: age through fear of surgery (β = −0.002, 95% CI −0.005, 0.001), monthly income through fear of diagnosis (β = −0.029, 95% CI −0.066, 0.007), monthly income through fear of surgery (β = 0.047, 95% CI −0.007, 0.100), monthly income through preference for a female physician (β = 0.026, 95% CI –0.008, 0.060), and education through fear of surgery (β = 0.072, 95% CI −0.001, 0.145) (Supplementary Material 1, wjon.elmerpub.com). In the structural model, several direct associations between sociodemographic characteristics and patient-perceived barriers reached statistical significance. Increased age was associated with lower fear of doctor or health-facility visits (β = −0.245, 95% CI −0.418, −0.071) and lower fear of surgery (β = −0.149, 95% CI −0.294, −0.003). Higher income (> 3 million Rupiah) was associated with lower fear of diagnosis (β = −0.128, 95% CI −0.225, −0.032), higher fear of surgery (β = 0.170, 95% CI 0.005, 0.334), and a greater likelihood of reporting preference for a female physician as a barrier (β = 0.161, 95% CI 0.046, 0.277). Lower educational attainment (no formal education to junior high school) was associated with higher fear of surgery (β = 0.283, 95% CI 0.104, 0.462). Being single, widowed, or divorced was associated with higher fear of cost (β = 0.383, 95% CI 0.184, 0.582) and lower reporting of CAM use as a first option (β = −0.130, 95% CI −0.224, −0.035). Six patient-perceived barriers were directly associated with presentation delay of more than 3 months: fear of diagnosis (β = 0.165, 95% CI 0.065, 0.264), fear of surgery (β = 0.247, 95% CI 0.099, 0.397), preference for a female physician (β = 0.105, 95% CI 0.020, 0.189), painless symptom (β = 0.367, 95% CI 0.223, 0.511), symptom minimization (β = 0.105, 95% CI 0.020, 0.189), and perceived busyness (β = 0.244, 95% CI 0.094, 0.394) (Supplementary Material 1, wjon.elmerpub.com).
| Discussion | ▴Top |
Growing evidence supports a strong association between delays in presentation, stage at diagnosis, and subsequent patient survival. Prolonged presentation intervals increase the likelihood of cancer being detected at an advanced stage, which is associated with poorer prognosis and reduced quality of life [2, 4]. Presentation delay reflects the interplay of multiple levels of determinants shaping health behavior. The interconnected layers of individual cognitive and emotional factors (awareness, health beliefs, emotional responses), social-environmental factors (work commitments, peer support, supportive networks), contextual factors (employment, income, education, healthcare access), and macro-level cultural and economic conditions collectively contribute to delays in presentation [12].
In our analysis, we found that the mediation model was not supported and that the findings are best interpreted as describing two sets of direct associations within a structural model. We have explored factors across these multiple layers and their interactions to better understand the complex thought processes underlying delayed presentation. Several sociodemographic variables were significantly associated with specific patient-perceived barriers. Multiple barriers also showed strong direct associations with delayed presentation. However, these perceived barriers did not significantly mediate the relationship between sociodemographic factors and presentation delay. This finding indicates that sociodemographic influences on delayed presentation do not operate through a single dominant mediating pathway, even when individual structural paths are significant. The individual effects of these barriers are insufficient in magnitude or consistency to produce statistically detectable mediation. Previous work has shown that statistical tests of indirect effects can have low power under realistic sample size and effect size conditions, making mediation difficult to detect even when structural paths exist [13]. The results also highlight that patient-perceived barriers are associated determinants of delayed presentation.
The overall model fit was mixed. Although the RMSEA and SRMR fell within commonly accepted thresholds, the CFI (0.732) and TLI (0.430) fell well below the conventional cutoffs. Several factors may contribute to this divergence, including low base rates in several patient-perceived barriers (e.g., “sought female physician” n = 2; “fear of cost” n = 4), which might produce sparse cross-classifications that disproportionately depress incremental fit. Furthermore, some relationships among barriers may be non-linear or moderated rather than additive, a possibility that the present specification does not capture. Accordingly, individual structural parameters can be interpreted as descriptive associations within the specified model, but the overall fit leaves substantive covariance unexplained and indicates a need for refinement in larger studies [14].
Sociodemographic factors and their influence on perceived barriers
In this study, older age was associated with lower fear of visiting health facilities and lower fear of surgery. The first finding contrasts with a previous report that 22.5% of adults avoided medical care due to examination-related discomfort and fear of serious illness [15], with these patterns modulated by health literacy [16]. In addition, older age was significantly associated with lower fear of surgery, consistent with prior evidence demonstrating a negative correlation between fear of surgery and age [17], plausibly reflecting the higher preoperative anxiety observed in younger patients [18]. These age-related differences may collectively reflect greater familiarity with healthcare settings, better emotional regulation, increased acceptance of medical interventions, and a greater readiness to confront health-related risks with advancing age [17, 18].
Higher income was linked to lower fear of cancer diagnosis, consistent with evidence that higher income reduces health anxiety [19] and less avoidance of serious illness [20]. Unexpectedly, higher income was also associated with greater fear of surgery, contrasting prior reports of greater preoperative anxiety among lower-income individuals due to financial concerns [21–23], which may reflect heightened expectations for treatment quality and outcomes among higher-income patients [24]. Higher-income patients also more frequently preferred female physicians, consistent with prior studies of provider gender preference [21–23], potentially reflecting the perception of female physicians as more empathetic [25], greater comfort during examination of intimate organs [25, 26], and the reinforcing influence of cultural norms in more conservative societies [26].
Lower educational attainment was associated with greater fear of surgery, consistent with evidence that limited health literacy elevates preoperative anxiety [27, 28], and that lower education correlates with anxiety in medical and surgical settings [18, 21, 29]. Higher education may attenuate this anxiety through cognitive and informational resources—critical thinking, access to health information, and understanding of procedures [18]. Being single, widowed, or divorced was associated with greater fear of healthcare costs and lower reporting of CAM as a barrier. The heightened cost-related fear plausibly reflects the financial vulnerability of unmarried women within reduced household financial support [30, 31], while the lower CAM reporting is consistent with evidence that married individuals are more likely to use CAM, possibly because of the shared decision-making and mutual support that marriage facilitates [32–34].
Patient-perceived barriers as factors associated with delayed presentation
Several patient-perceived barriers were associated with delayed presentation in the model. Among the most prominent barriers was fear of a cancer diagnosis, which is a known psychological reason that makes people delay seeking help. Finding from previous study shows that 34% of women waited to get care because they were afraid of being told that they had BC [35]. This fear may come from worries about dying after a cancer diagnosis, which can make people avoid care or put off seeking care [36].
Fear of surgery was found to be a substantial barrier, particularly in the context of BC. Fears of diminished sexuality, loss of femininity, or altered self-worth related to breast surgery might delay patients’ presentation [37, 38]. Evidence suggests that preoperative psychosocial screening and supportive interventions may help reduce these fears [39]. Cognitive barriers, such as perceiving painless symptoms and symptom minimization, were frequently reported. Patients may misinterpret painless breast lumps as benign or self-limiting and delay medical presentation, as patients assume that symptoms will resolve [5, 38]. This highlights persistent gaps in public awareness of BC symptoms and underscores the need for targeted educational initiatives [40, 41].
In addition, practical and culturally specific barriers were significantly associated with delayed presentation, with perceived busyness serving as a key factor. This sense of busyness, especially due to competing work and family responsibilities, often leads individuals to deprioritize their health [42]. This calls attention to the need for more flexible healthcare delivery models, such as extended clinic hours and mobile health services [43].
Finally, preference for female physicians emerged as a key barrier for some participants, as women might delay or avoid medical consultations when female healthcare providers are unavailable. This is particularly pronounced in Indonesian women, where cultural and religious norms strongly influence healthcare-seeking behaviors [44–46]. Addressing this barrier requires system-level responses. Improving the availability of female providers and integrating culturally competent care that respects patient preferences, beliefs, and religious practices can increase trust, patient satisfaction, and timely access to care [47, 48].
Strength and limitations
This study applies a theory-driven path analysis to examine complex relationships between sociodemographic characteristics, patient-perceived barriers, and delayed BC presentation, enabling a nuanced understanding of how distal and proximal factors might interact. By incorporating a broad range of patient-perceived barriers across cognitive, emotional, and cultural dimensions, the analysis moves beyond isolated factors to capture the multifaceted nature of help-seeking behavior, thereby providing empirically grounded insights to inform targeted interventions that address modifiable patient-level barriers alongside sociodemographic context.
Several limitations should be acknowledged. This study was conducted at a single center, which may limit generalizability, and further multicenter studies are required to confirm these findings. The modest sample size in this study, relative to the complexity of the path model, limited statistical power for detecting indirect effects, which is a recognized challenge in mediation analysis when constituent paths are of small-to-moderate magnitude [13]. Larger multicenter studies are warranted to further confirm the absence of mediation in the hypothesized model.
Additionally, although efforts to anchor recall to events or dates have been made through the use of recall protocols [8], self-reported data on timing and intervals, and reasons for delay as patient-perceived barriers, may still be affected by recall bias and recall uncertainty cannot be fully eliminated. Recall could also be selectively distorted by the emotional salience of the subsequent cancer diagnosis or surgery, producing either “compression” or “telescoping” of recalled intervals [49]. Moreover, since patient-perceived barriers were assessed retrospectively, some reported barriers may represent post hoc rationalizations [50].
Patient-perceived barriers were assessed using single-item categorical responses derived from open-ended interview content rather than validated psychometric instruments. Multidimensional constructs (e.g., fear of diagnosis or fear of surgery) are represented as binary indicators that capture the presence of the concern as a stated reason for delay but not its intensity, duration, or specific cognitive content. Additionally, since themes mentioned by only a single participant were excluded in order to avoid unstable parameters, the exclusion may have removed some idiosyncratic but potentially meaningful barriers. Future qualitative studies with larger samples would be better positioned to examine these lower-frequency responses.
Because the data are cross-sectional and barriers were assessed retrospectively, temporal ordering between barriers and presentation delay was not established, and the path-analytic findings should therefore be interpreted as exploratory associations within a hypothesized structural model rather than as evidence of causal pathways. In addition, the presumed directionality between perceived barriers and presentation delay may be bidirectional, a relationship that has not been evaluated in this study.
Conclusions
This study shows that patient-perceived barriers are associated with delayed BC presentation. While sociodemographic factors were associated with specific barriers, these barriers did not significantly mediate the association between sociodemographic characteristics and presentation delay, which is shown in the non-significant indirect effect in the hypothesized model. These suggest that sociodemographic influences might not act through a single dominant pathway. Rather, the findings indicate that patient-perceived barriers operate as factors associated with delayed presentation within the modelled framework of delayed presentation across different sociodemographic groups. Addressing these modifiable cognitive, emotional, practical, and cultural barriers may therefore be important for promoting earlier presentation and improving BC outcomes.
| Supplementary Material | ▴Top |
Suppl 1. Direct and indirect effects of sociodemographic factors and patient-perceived barriers on delayed breast cancer presentation.
Acknowledgments
We gratefully thanked Mentari Widiastuti and Norma Dewi Suryani for technical assistance.
Financial Disclosure
This study was supported by Kementrian Riset, Teknologi dan Pendidikan Tinggi Republik Indonesia (2018) and Faculty of Medicine, Public Health, and Nursing, Universitas Gadjah Mada, Yogyakarta, Indonesia (2021).
Conflict of Interest
The authors declare they have no competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Informed Consent
Written informed consent was obtained from all participants.
Author Contributions
Juan Adrian Wiranata: conceptualization, data acquisition, formal analysis, data interpretation, writing – original draft. Susanna Hilda Hutajulu: conceptualization, resources, supervision, data acquisition, formal analysis, data interpretation, writing – review and editing. Yufi Kartika Astari: data acquisition, data interpretation. Angelica Abigael: data interpretation, writing – original draft. Mardiah Suci Hardianti: resources, supervision, data acquisition. Kartika Widayati Taroeno-Hariadi: resources, supervision, data acquisition. Johan Kurnianda: resources, supervision, data acquisition. Yayi Suryo Prabandari: formal analysis, data interpretation, writing – review and editing. Ibnu Purwanto: resources, supervision, data acquisition.
Data Availability
Any inquiries regarding supporting data availability of this study should be directed to the corresponding author.
Abbreviations
BC: breast cancer; CAM: complementary and alternative medicines; CFI: Comparative Fit Index; CI: confidence interval; ECOG: Eastern Cooperative Oncology Group; RMSEA: root mean square error of approximation; SRMR: standardized root mean square residual; TLI: Tucker–Lewis Index
| References | ▴Top |
- Bray F, Laversanne M, Sung H, Ferlay J, Siegel RL, Soerjomataram I, Jemal A. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2024;74(3):229-263.
doi pubmed - Hutajulu SH, Prabandari YS, Bintoro BS, Wiranata JA, Widiastuti M, Suryani ND, Saptari RG, et al. Delays in the presentation and diagnosis of women with breast cancer in Yogyakarta, Indonesia: A retrospective observational study. PLoS One. 2022;17(1):e0262468.
doi pubmed - Sinaga ES, Ahmad RA, Shivalli S, Hutajulu SH. Age at diagnosis predicted survival outcome of female patients with breast cancer at a tertiary hospital in Yogyakarta, Indonesia. Pan Afr Med J. 2018;31:163.
doi pubmed - Wendimu DE, Degefa MB, Achalu DL, Mamo BT, Daba DB, Meshesha SG. Timeliness of breast cancer patients' presentation to health care facilities in Ethiopia: a systematic review and meta-analysis. JCO Glob Oncol. 2024;10:e2400263.
doi pubmed - Mulugeta C, Emagneneh T, Kumie G, Ejigu B, Alamrew A. Delayed presentation of breast cancer patients and contributing factors in East Africa: Systematic review and meta-analysis. PLoS One. 2024;19(11):e0309792.
doi pubmed - Streiner DL. Finding our way: an introduction to path analysis. Can J Psychiatry. 2005;50(2):115-122.
doi pubmed - Suchaini U, Nugraha WPS, Dwipayana IKD, Lestari SA. Indeks Kebahagiaan 2021. Badan Pusat Statistik RI; 2021.
- Neal RD, Nafees S, Pasterfield D, Hood K, Hendry M, Gollins S, Makin M, et al. Patient-reported measurement of time to diagnosis in cancer: development of the Cancer Symptom Interval Measure (C-SIM) and randomised controlled trial of method of delivery. BMC Health Serv Res. 2014;14:3.
doi pubmed - Braun V, Clarke V. Using thematic analysis in psychology. Qualitative Research in Psychology. 2006;3:77-101.
doi - Kline RB. Principles and practice of structural equation modeling. Guilford Publications; 2023.
- MacKinnon DP, Lockwood CM, Hoffman JM, West SG, Sheets V. A comparison of methods to test mediation and other intervening variable effects. Psychol Methods. 2002;7(1):83-104.
doi pubmed - Hoveling LA, Schuurman M, Siesling S, van Asselt KM, Bode C. Diagnostic delay in women with cancer: What do we know and which factors contribute? Breast. 2025;80:104427.
doi pubmed - Fritz MS, Mackinnon DP. Required sample size to detect the mediated effect. Psychol Sci. 2007;18(3):233-239.
doi pubmed - Hu L, Bentler PM. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Structural Equation Modeling: A Multidisciplinary Journal. 1999;6:1-55.
doi - Leyva B, Taber JM, Trivedi AN. Medical care avoidance among older adults. J Appl Gerontol. 2020;39(1):74-85.
doi pubmed - Xu J, Xia C, Ding X. Does health literacy affect older people's avoidance of medical care? The sense of medical care policy alienation and perceptions of control. Geriatr Nurs. 2023;51:202-208.
doi pubmed - Akutay S, Ceyhan O. The relationship between fear of surgery and affecting factors in surgical patients. Perioper Med (Lond). 2023;12(1):22.
doi pubmed - Goyal P, Prisha, Chacko JS, Goyal A, Gupta S, Kathuria S. Assessment of perioperative anxiety levels at three time-points during hospital stay in patients undergoing elective surgery. Perioper Med (Lond). 2025;14(1):27.
doi pubmed - Barbek RME, Makowski AC, von dem Knesebeck O. Social inequalities in health anxiety: A systematic review and meta-analysis. J Psychosom Res. 2022;153:110706.
doi pubmed - Benke C, Wallenfels LM, Bleichhardt GM, Melzig CA. Health anxiety amplifies fearful responses to illness-related imagery. Sci Rep. 2024;14(1):4345.
doi pubmed - Bedaso A, Mekonnen N, Duko B. Prevalence and factors associated with preoperative anxiety among patients undergoing surgery in low-income and middle-income countries: a systematic review and meta-analysis. BMJ Open. 2022;12(3):e058187.
doi pubmed - YB W, Gl F, Ht Y, Ag H. Prevalence and factors associated with preoperative anxiety among elective surgical patients at University of Gondar Hospital. Gondar, Northwest Ethiopia, 2017. A cross-sectional study. International Journal of Surgery Open 2018;10:21-29.
doi - Topal Hancer A. Prevalence and factors associated with surgery anxiety in hospitalized patients: a point-prevalence study. Ir J Med Sci. 2023;192(5):2095-2103.
doi pubmed - Nigussie S, Belachew T, Wolancho W. Predictors of preoperative anxiety among surgical patients in Jimma University Specialized Teaching Hospital, South Western Ethiopia. BMC Surg. 2014;14:67.
doi pubmed - Zaghloul AA, Youssef AA, El-Einein NY. Patient preference for providers' gender at a primary health care setting in Alexandria, Egypt. Saudi Med J. 2005;26(1):90-95.
pubmed - Kitole FA, Ali Z, Song J, Ali M, Fahlevi M, Aljuaid M, Heidler P, et al. Exploring the gender preferences for healthcare providers and their influence on patient satisfaction. Healthcare (Basel). 2025;13(9):1063.
doi pubmed - Demirel A, Balkaya AN, Onur T, Karaca U, Onur A. The effect of health literacy on preoperative anxiety levels in patients undergoing elective surgery. Patient Prefer Adherence. 2023;17:1949-1961.
doi pubmed - Anar EN, Kirtil I. Relationship between preoperative surgical fear, anxiety, and satisfaction levels in individuals choosing bariatric surgery tourism: a descriptive, cross-sectional study. Obes Surg. 2025;35(4):1326-1336.
doi pubmed - Nuri A, Abute L, Tesfaye Elilo L, Dejene Y, Ali S, Mezgebu T, Hailu M, et al. Assessment of preoperative anxiety levels among patients admitted for surgery in public hospitals, Southern Ethiopia. SAGE Open Nurs. 2024;10:23779608241274191.
doi pubmed - Azubuike CD, Alawode OA. Delayed healthcare due to cost among adults with multimorbidity in the United States. Healthcare (Basel). 2024;12(22):2271.
doi pubmed - Hinata H, Lwin KS, Eguchi A, Ghaznavi C, Hashizume M, Nomura S. Factors associated with barriers to healthcare access among ever-married women of reproductive age in Bangladesh: Analysis from the 2017-2018 Bangladesh Demographic and Health Survey. PLoS One. 2024;19(1):e0289324.
doi pubmed - Ben Salah G, Alyousef M, Alresheedi L, Alharbi R, Alazzaz S, Alanazi S, et al. The utilization of complementary and alternative medicine among adults in Al Qassim Region, Saudi Arabia: a cross-sectional study. Open Public Health J. 2025;18.
doi - Almouaalamy NA, Banjar LA, Alshaikh HM, Altowairqi JM, Alharbi NM, Alghamdi WA. The prevalence and pattern of complementary and alternative medicine use among cancer patients in a tertiary oncology center: a cross-sectional study. Ann Med Surg (Lond). 2023;85(11):5420-5427.
doi pubmed - Zhang Y, Leach MJ, Hall H, Sundberg T, Ward L, Sibbritt D, Adams J. Differences between male and female consumers of complementary and alternative medicine in a national US population: a secondary analysis of 2012 NIHS data. Evid Based Complement Alternat Med. 2015;2015:413173.
doi pubmed - Abo Al-Shiekh SS, Alajerami YS, Abushab KM, Najim AA, AlWaheidi S, Davies EA. Factors affecting delay in the presentation of breast cancer symptoms among women in Gaza, occupied Palestinian territory: a cross-sectional survey. BMJ Open. 2022;12(10):e061847.
doi pubmed - Kumar A, Bhagabaty SM, Tripathy JP, Selvaraj K, Purkayastha J, Singh R. Delays in diagnosis and treatment of breast cancer and the pathways of care: a mixed methods study from a tertiary cancer centre in North East India. Asian Pac J Cancer Prev. 2019;20(12):3711-3721.
doi pubmed - Saeed S, Asim M, Sohail MM. Fears and barriers: problems in breast cancer diagnosis and treatment in Pakistan. BMC Womens Health. 2021;21(1):151.
doi pubmed - Martei YM, Vanderpuye V, Jones BA. Fear of mastectomy associated with delayed breast cancer presentation among ghanaian women. Oncologist. 2018;23(12):1446-1452.
doi pubmed - Taurisano P, Abbatantuono C, Verri V, Pepe I, Stucci LS, Taurino A, Moschetta M, et al. Pre-surgery supportive and goal-oriented strategies are associated with lower post-surgery perceived distress in women diagnosed with breast cancer. BMC Psychol. 2022;10(1):2.
doi pubmed - Koo MM, von Wagner C, Abel GA, McPhail S, Rubin GP, Lyratzopoulos G. Typical and atypical presenting symptoms of breast cancer and their associations with diagnostic intervals: Evidence from a national audit of cancer diagnosis. Cancer Epidemiol. 2017;48:140-146.
doi pubmed - Chao CA, Huang L, Visvanathan K, Mwakatobe K, Masalu N, Rositch AF. Understanding women's perspectives on breast cancer is essential for cancer control: knowledge, risk awareness, and care-seeking in Mwanza, Tanzania. BMC Public Health. 2020;20(1):930.
doi pubmed - Dedey F, Nsaful J, Brownson KE, Laryea RY, Coleman N, Tetteh J, Clegg-Lamptey JN, et al. Health-seeking behaviour of breast cancer patients receiving care at a tertiary institution in Ghana. Ecancermedicalscience. 2024;18:1756.
doi pubmed - Alissa NA. A cross-sectional study on healthcare seeking behavior among Saudi women in Riyadh. Sci Rep. 2025;15(1):9497.
doi pubmed - Vu M, Azmat A, Radejko T, Padela AI. Predictors of delayed healthcare seeking among American Muslim women. J Womens Health (Larchmt). 2016;25(6):586-593.
doi pubmed - Alqufly AE, Alharbi BM, Alhatlany KK, Alhajjaj FS. Muslim female gender preference in delaying the medical care at emergency department in Qassim Region, Saudi Arabia. J Family Med Prim Care. 2019;8(5):1658-1663.
doi pubmed - Afsah YR, Kaneko N. Exploring cervical cancer screening awareness, beliefs, barriers, and practices among indonesian muslim women in Japan: a qualitative study. BMC Public Health. 2025;25(1):1084.
doi pubmed - Alhomayani KM, Bukhary HA, Aljuaid FI, Alotaibi TA, Alqurashi FS, Althobaiti KN, Althobaiti NS, et al. Gender preferences in healthcare: a study of Saudi patients' physician preferences. Patient Prefer Adherence. 2025;19:295-303.
doi pubmed - Tackett S, Young JH, Putman S, Wiener C, Deruggiero K, Bayram JD. Barriers to healthcare among Muslim women: a narrative review of the literature. Women’s Studies International Forum. 2018;69:190-194.
doi - Rubin DC, Baddeley AD. Telescoping is not time compression: a model of the dating of autobiographical events. Mem Cognit. 1989;17(6):653-661.
doi pubmed - Coughlin SS. Recall bias in epidemiologic studies. J Clin Epidemiol. 1990;43(1):87-91.
doi pubmed
This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (CC BY 4.0), which permits unrestricted use, distribution, and reproduction in any medium, including commercial use, provided the original work is properly cited.
World Journal of Oncology is published by Elmer Press Inc.