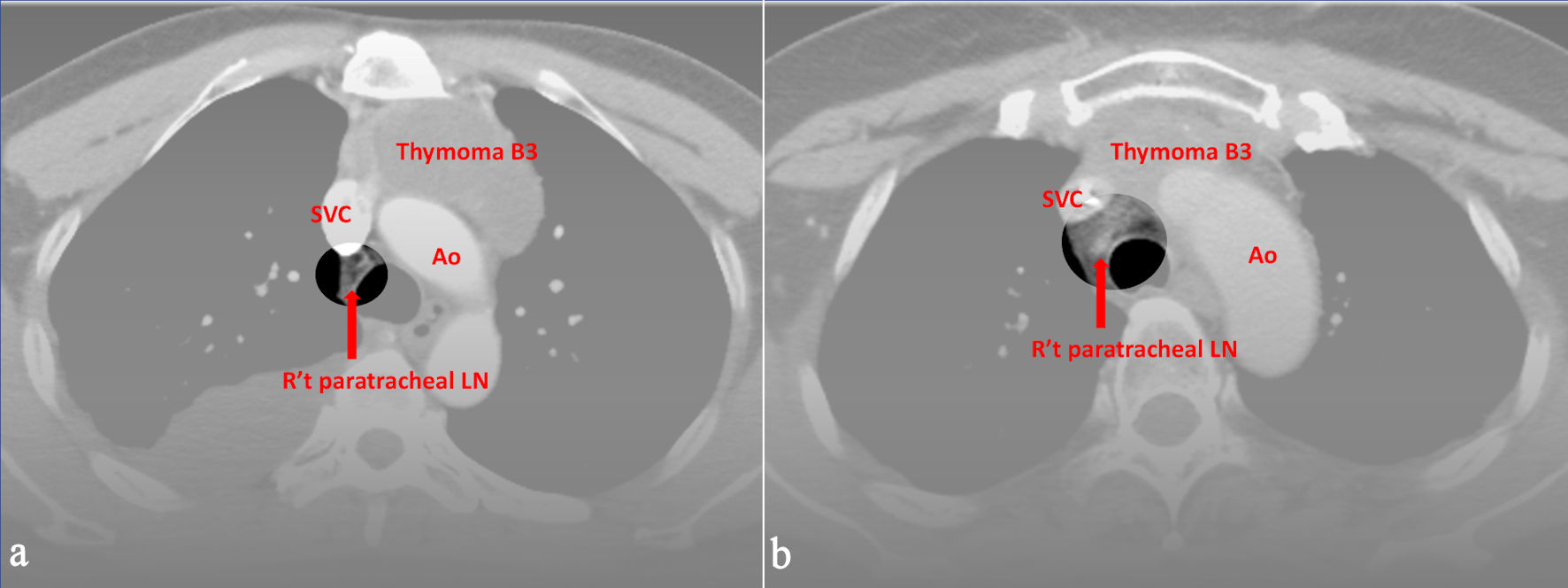
↓ Figure 1. Preoperative CT images of (a) a 52-year-old male and (b) a 49-year-old female with World Health Organization (WHO) classification B3. All three radiologists evaluated right upper paratracheal LN metastasis, and the pathological report proved the positive findings. Ao: aorta; SVC: superior vena cava; CT: computed tomography; LN: lymph node.
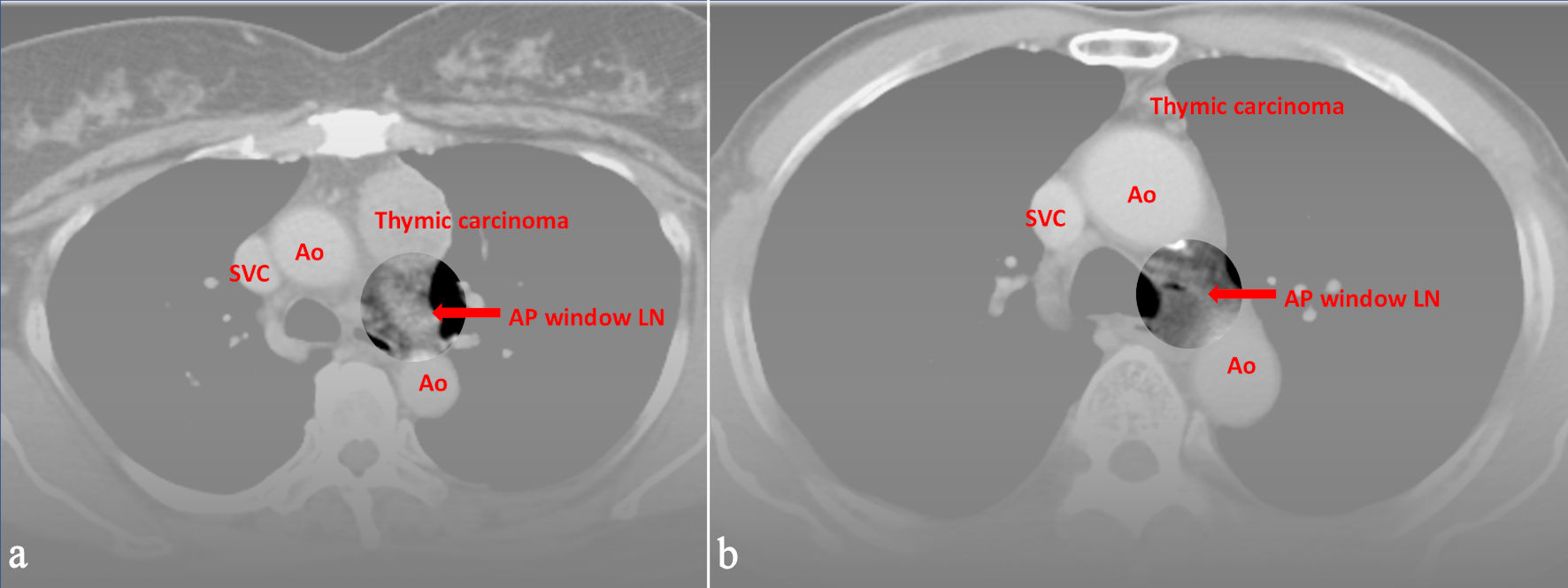
↓ Figure 2. Preoperative CT images of (a) a 59-year-old female and (b) a 74-year-old male with World Health Organization (WHO) classification thymic carcinoma. All three radiologists evaluated LN metastasis in the aortopulmonary window, and the pathological report proved the positive findings. Ao: aorta; SVC: superior vena cava; CT: computed tomography; LN: lymph node.