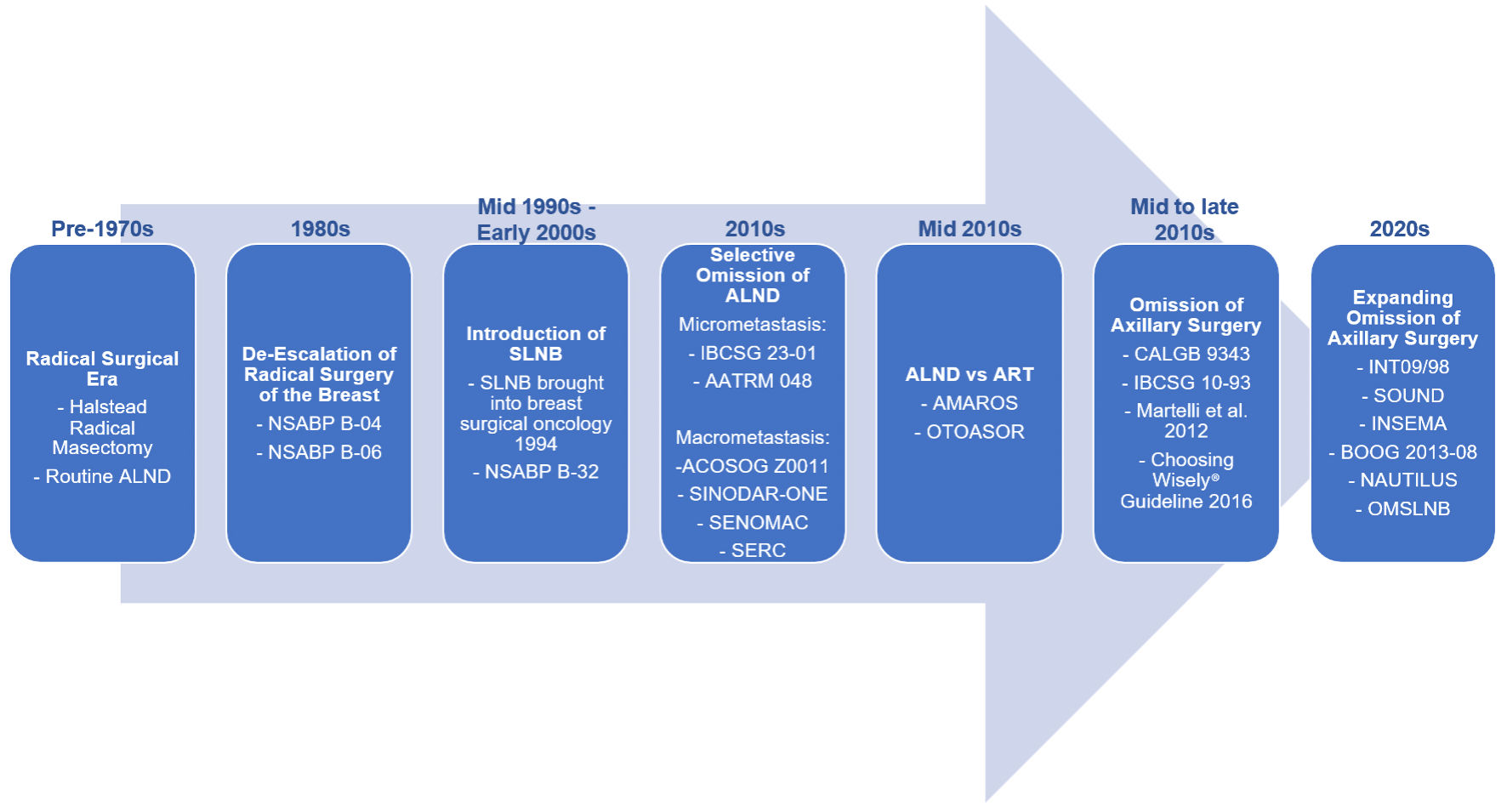
↓ Figure 1. Evolution of axillary management in breast cancer. Axillary surgery has progressively de-escalated from routine axillary lymph node dissection (ALND) toward sentinel lymph node biopsy (SLNB), and more recently, omission of axillary surgery in selected patients. Landmark trials, including NSABP B-04 [15], NSABP B-06 [16], NSABP B-32 [5], IBCSG 23-01 [1], AATRM 048 [6], ACOSOG Z0011 [4], SINODAR-ONE [27], SENOMAC [28], SERC [29], AMAROS [31], OTOASOR [30], CALGB 9343 [8], IBCSG 10-93 [9], Martelli et al (2012) [32], INT09/98 [17], SOUND [33], and INSEMA [34], have established the safety of reducing surgical intervention without compromising oncologic outcomes. BOOG 2013-08 [35], NAUTILUS [36], and OMSLNB [37] trials are ongoing to confirm preliminary findings of SOUND and INSEMA expanding the population of women eligible for omission of axillary surgery. NSABP: National Surgical Adjuvant Breast and Bowel Project; IBCSG: International Breast Cancer Study Group; AMAROS: After Mapping of the Axilla: Radiotherapy or Surgery; OTOASOR: Optimal Treatment of the Axilla- Surgery Or Radiotherapy; SOUND: Sentinel Node vs. Observation After Axillary Ultra-Sound; INSEMA: Intergroup Sentinel Mamma; CALGB: Cancer and Leukemia Group B.