| Flap name |
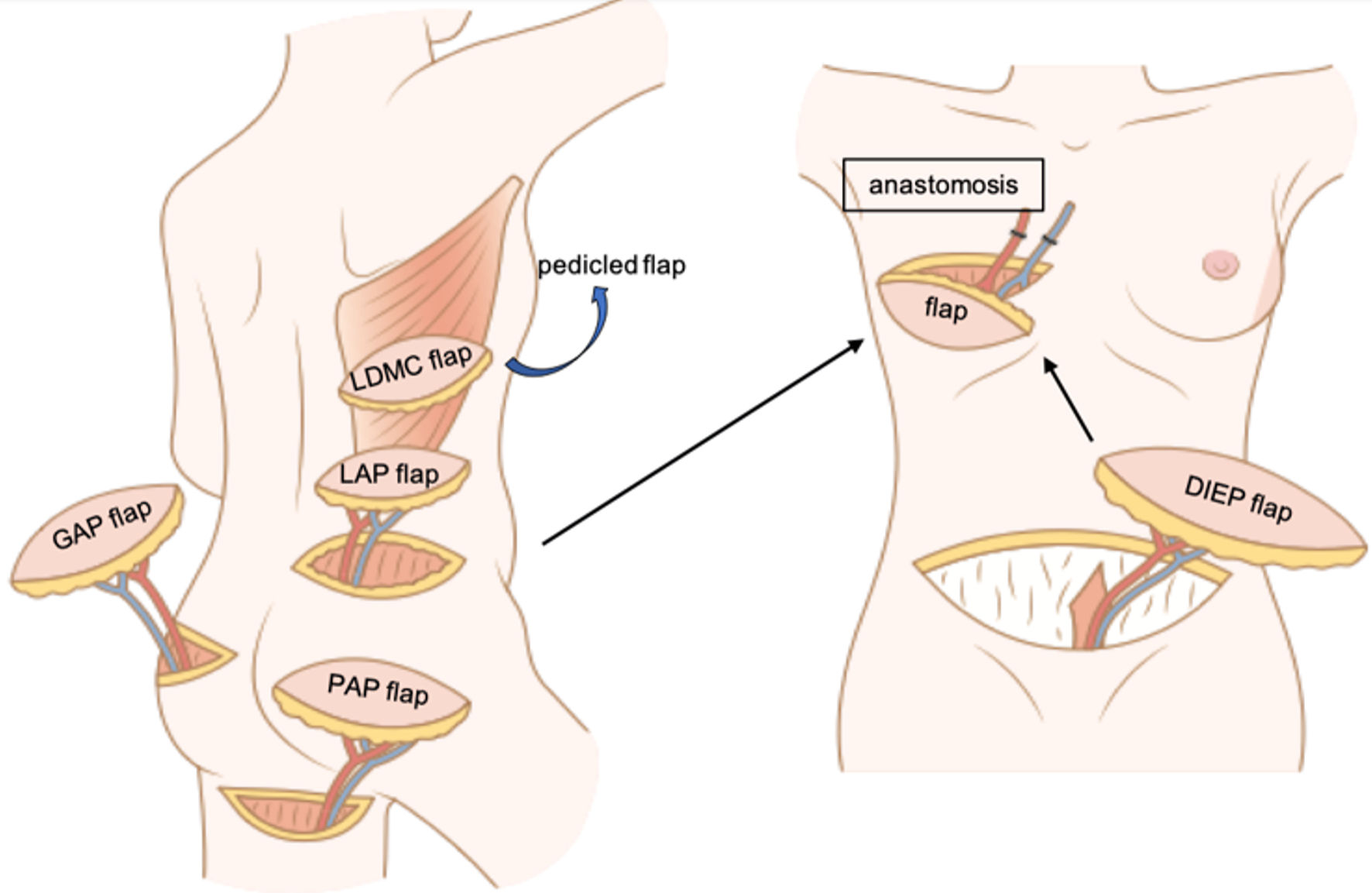
LDMC flap [66] |
LAP flap [58] |
DIEP flap [68] |
TRAM flap [69] |
PAP flap [56] |
GAP flap [55, 62] |
| Flap type |
Myocutaneous flap |
Perforator flap |
Perforator flap |
Myocutaneous flap |
Perforator flap |
Perforator flap |
| Patient selection criteria |
Small breast |
Large breast (for salvage) |
Large breast |
Small to medium breast |
Large breast (alternative for DIEP flap) |
|
|
|
Exclusion criteria: desire to have a baby, complicated
surgical scars in the abdomen, history of abdominoplasty |
|
|
| Advantages |
Does not require: 1) vascular anastomosis; 2) dissection of perforator
|
Ease of elevation
Well-concealed scar
Muscle sparing |
Large volume so flexibility for breast
mound
Abdominoplasty |
Muscle sparing
Inconspicuous scar |
Large volume
Muscle sparing |
|
|
|
Muscle sparing
Less hernia and bulging [54] (than TRAM flap) |
Does not require: 1) vascular anastomosis (pedicled TRAM flap);
2)
dissection of perforator |
|
|
| Disadvantages |
Small volume
Volume loss due to muscle atrophy
Intraoperative
repositioning
Conspicuous scar |
Intraoperative repositioning
Short pedicle [67] |
Conspicuous scar |
Small volume |
Short pedicle [70] |
|
|
|
Requires: 1) vascular anastomosis; 2) dissection of perforator |
Volume loss due to muscle atrophy
Hernia and bulging |
Requires: 1) vascular anastomosis; 2) dissection of perforator |
Intraoperative repositioning
Requires: 1) vascular anastomosis; 2)
dissection of perforator |